

AXIS I
4. ASSOCIATED FEATURES
From: Albanese A, Di Giovanni M, Lalli S. Dystonia: diagnosis and management. Eur J Neurol. 2019;26(1):5-17. doi:10.1111/ene.13762
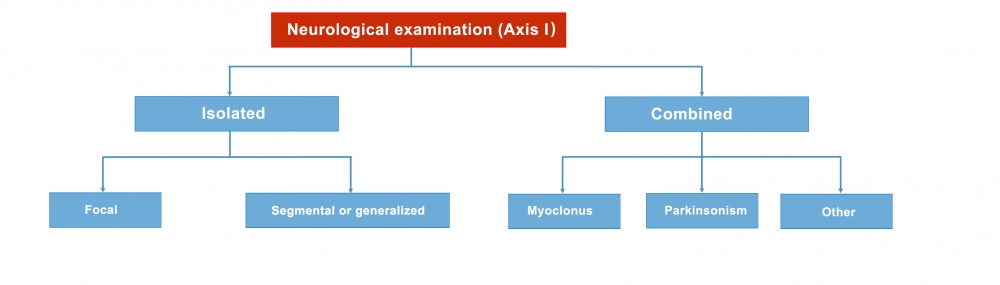
Axis I, the clinical characteristics of dystonia, includes the category of Associated Features. Dystonia may be isolated or combined with other movement disorders, such as parkinsonism or myoclonus. This is important for determining the syndromic pattern, and this category of Associated Features may be divided into:
In isolated dystonia, dystonia is the only motor feature, with the exception of tremor. (This category includes most cases previously described as described as “pure” or “primary”).
In combined dystonia, dystonia is combined with other movement disorders (such as myoclonus, parkinsonism, etc). (This category includes most cases previously described as “dystonia plus” or “heredodegenerative”).
The term combined dystonia refers to syndromes in which dystonia is combined with other clinical problems. It may be combined with other movement disorders, such as parkinsonism or ataxia, with other neurologic problems, such as retinopathy, deafness, dementia, or neuropathy or with systemic issues, such as liver or kidney disease1.
In combined forms, dystonia does not necessarily have to be the predominant movement disorder.
- Chorea produces movements that vary randomly in duration, direction, and amplitude (rather than movements that are patterned or stereotyped).
- Myoclonus. Dystonia can cause rapid, jerky movements that can be confused with myoclonus. When myoclonus coexists with dystonia, it will usually be present not only in parts of the body affected by dystonia, but also in non-affected parts.
- Athetosis is a movement disorder that occurs in the setting of dystonia and can be confused with tremor, chorea, or myoclonus. Athetosis refers to repetitive movements of variable speed and frequency that independently affect individual (but usually multiple) fingers, toes, and facial muscles2.