

Horizontal canal BPV is a far less common cause of positional vertigo and is best evoked by the supine roll test, which should detect a canalolithiasis or cupulolithiasis of the horizontal canal.
In addition, lateral semicircular canal BPPV tends to self-resolve more quickly than posterior semicircular canal BPPV1.
When the horizontal canal is affected, characteristics of nystagmus include:
- No latency
- Purely horizontal
- Responses do not fatigue
- The duration may be greater than 60 seconds
- The nystagmus often changes direction after a brief nystagmus-free interval, if the head is maintained in the testing position. If this occurs, the direction of the initial nystagmus should be used to determine the mechanism and affected ear2.
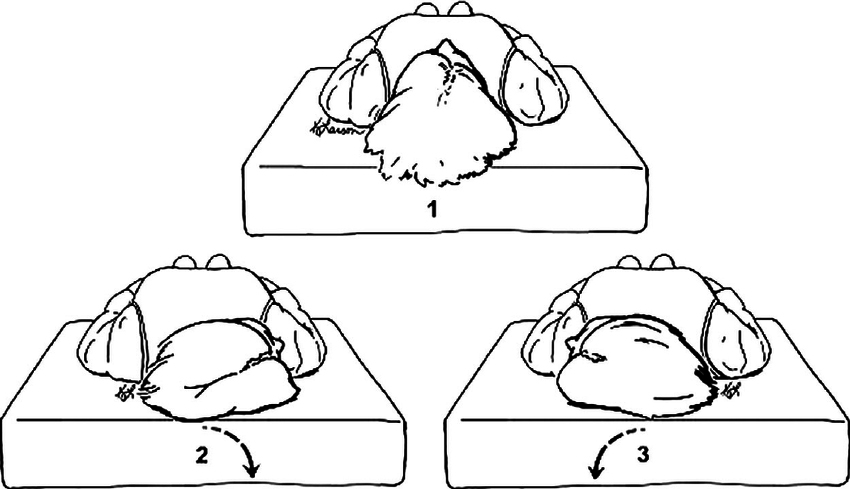
The test begins with the subject flat, with their head raised on a single pillow, in order that the head is elevated 30 degrees from horizontal (in which position the horizontal canals are vertical).
The patient’s head is rotated 90 degrees, first to one side, and then to the other, looking for the development of horizontal nystagmus. Note that if significant horizontal nystagmus occurs without the subjective experience of vertigo, a central cause of positional nystagmus should be suspected).
From: Fife TD, Iverson DJ, Lempert T, et al. Practice parameter: therapies for benign paroxysmal positional vertigo (an evidence-based review): report of the Quality Standards Subcommittee of the American Academy of Neurology. Neurology. 2008;70(22):2067-2074.
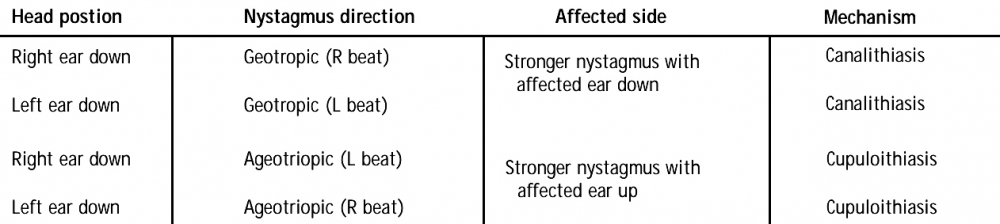
Two potential nystagmus findings may occur with this manoeuvre, reflecting two types of lateral semicircular canal BPPV. The types are geotropic and apogeotropic, representing canalithiasis and cupulolithiasis respectively.
Both types are characterised by so-called direction-changing positional nystagmus: that is, the direction of the positional nystagmus changes with changes in the head position.
Canalithiasis: (example, right horizontal semicircular canal involvement)
-Rotating to the affected right side provokes a paroxysm of horizontal geotropic nystagmus beating towards the ear which is down (the right ear).
When lying on the affected right side, the otoconia drift towards the ampulla. For the horizontal canal, ampullopetal movement of the cupula is excitatory and results in right-beating nystagmus.
-Rotating to the left provokes a similar but less intense paroxysm, which again beats down, in this case, to the left ear.
When lying on the unaffected left side, the otoconia drift ampullofugally and inhibit the right horizontal canal afferents, and inhibitory (left-beating) nystagmus follows.
Horizontal canal BPPV can also show spontaneous horizontal nystagmus in the sitting position that reverses direction when putting the head forward (’bow and lean’ nystagmus). This may help to identify the pathological side when the intensity of the nystagmus does not change depending upon which ear is down (in canalolithiasis in the supine right or left head roll test the nystagmus is most intense when it is beating toward the pathological ear)3.
Cupulolithiasis: the calcium carbonate debris is located adherent to or close to the ampulla of the semicircular canal4.
In this case, the supine roll test results in a horizontal nystagmus beating toward the uppermost ear (apogeotropic nystagmus). Upon rolling to the opposite side, the nystagmus will change direction, again beating toward the uppermost ear.
In the case of cupulolithiasis, rotating the head toward the affected side will cause gravity to deflect the cupula towards the canal, which is inhibitory, thereby resulting in nystagmus beating away from the dependent ear (apogeotropic). When the affected ear is upward, the cupula is deflected in the excitatory direction, and therefore a stronger (still apogeotropic) nystagmus is observed2.
From: Solomon D. Benign Paroxysmal Positional Vertigo. Curr Treat Options Neurol. 2000;2(5):417-428. doi:10.1007/s11940-000-0040-z
With the unaffected right ear down, a paroxysm of right-beating horizontal positional nystagmus is seen.
With the affected left ear down, a higher velocity paroxysm of left-beating horizontal positional nystagmus is seen.
(vv)BaranyHorizontalcanalbppv.mp4(tt)
From: Committee for the International Classification of Vestibular Disorders of the Barany Society.2.3.1.1.2. Horizontal semicircular canal benign paroxysmal positional nystagmus. Retrieved from http://www.jvr-web.org/images/2.3.1.1.2.-Horizontal-canal-BPPV.m4v
(vv)GEO.mp4(tt)
From: Straumann D. How to diagnose and treat benign paroxysmal positional vertigo. EAN 2020
(vv)APOGeo.mp4(tt)
From: Straumann D. How to diagnose and treat benign paroxysmal positional vertigo. EAN 2020
(vv)HorBPPV.mp4(tt)
From: Halmagyi GM. Clinical Examination of the Vestibular System. J Vestib Res. Teaching Course, 29th Bárány Society Meeting, Lecture 2, June 5, 2016, Seoul, Korea.
From: https://www.youtube.com/watch?v=ehR7SOlBBow
Horizontal canal BPPV can be treated with the Gufoni manoeuvre, for both canalolithiasis and cupulolithiasis.
To correctly identify the affected ear, nystagmus intensity with either ear down can be compared4. For the geotropic variant: the affected labyrinth is on the side of the strongest nystagmus (follows Ewald's second law, whereby stimulation is more effective in inducing a vestibular response than inhibition). For the apogeotropic variant, the affected labyrinth is on the side of the weaker nystagmus5.
When determination of the involved side using the Ewald’s second law is difficult due to fairly symmetrical responses during the supine roll test, the direction of lying-down nystagmus (LDN) or head-bending nystagmus (HBN) may help. In geotropic horizontal canal-BPPV, LDN beats mostly toward the intact side, while HBN is directed to the affected side. By contrast, LDN is usually ipsilesional and HBN is mostly contralesional in the apogeotropic form. Patients with apogeotropic horizontal canal-BPPV may have a null head position in which the induced horizontal nystagmus disappears or becomes minimal. The null position is usually found when the head is turned to the affected side by 10-20°.

From: Huh YE, Kim JS. Bedside evaluation of dizzy patients. J Clin Neurol. 2013;9(4):203-213. doi:10.3988/jcn.2013.9.4.203
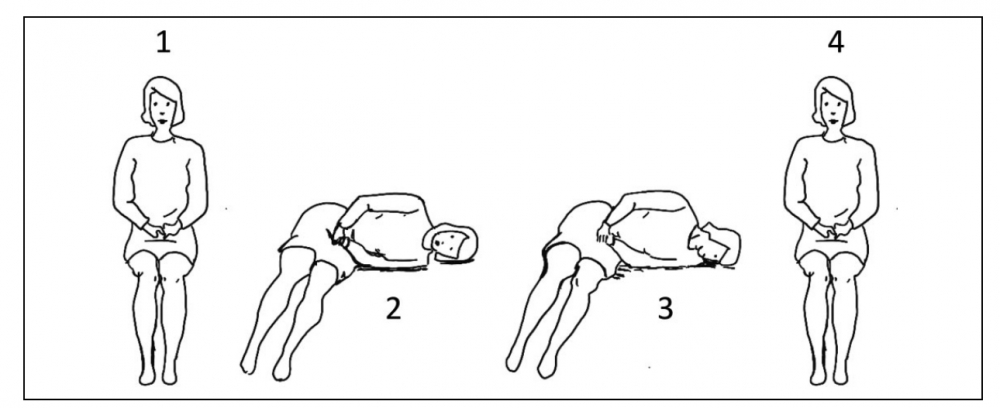
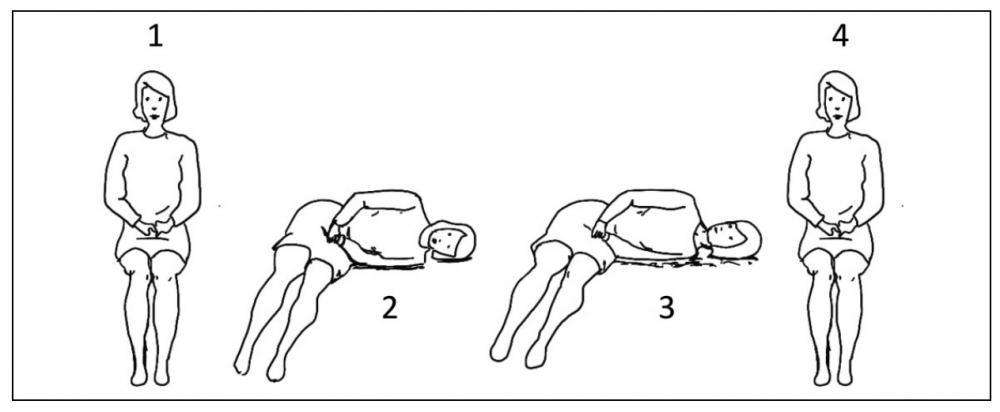
There are two versions of the Gufoni liberation maneuver: one for the geotropic variant (Figure 2) and one for the apogeotropic variant (Figure 3) of horizontal BPPV.
- In both versions, the patient is seated upright on the side of the examination table (Figures 2 and 3, position 1)
- The patient is fhen placed so as to be lying on their side (Figures 2 and 3, position 2). (The side chosen is that which had the least amount of horizontal positional nystagmus during the supine-roll provocation manoeuvre ).
- In the case of the geotropic variant, this is the side of the unaffected ear; in the case of the apogeotropic variant, this is the side of the affected ear.
- After 20 seconds in this side position, the head is rotated in the yaw plane 45 degrees down (Figure 2, position 3) for the geotropic variant or 45 degrees up (Figure 3, position 3) for the apogeotropic variant.
- After 1–2 min in this position, the patient is brought back to the sitting position,and the head may rotate back to the neutral position (Figures 2 and 3, position 4).
(vv)Lateral SemiCC.mp4(tt)
From: Straumann D. How to diagnose and treat benign paroxysmal positional vertigo. EAN 2020
(vv)Gufoni Head Up-3.mp4(tt)
From: Straumann D. How to diagnose and treat benign paroxysmal positional vertigo. EAN 2020
(vv)Gufon Head Downi.mp4(tt)
From: Straumann D. How to diagnose and treat benign paroxysmal positional vertigo. EAN 2020