

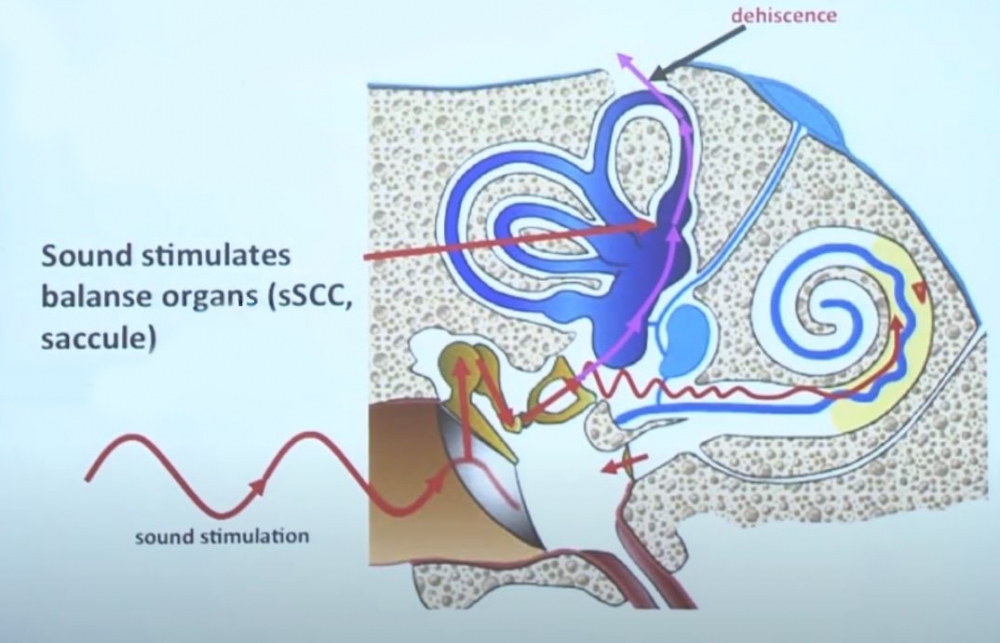
In addition to the oval and round windows, a defect in the bony labyrinth can function as a third window.
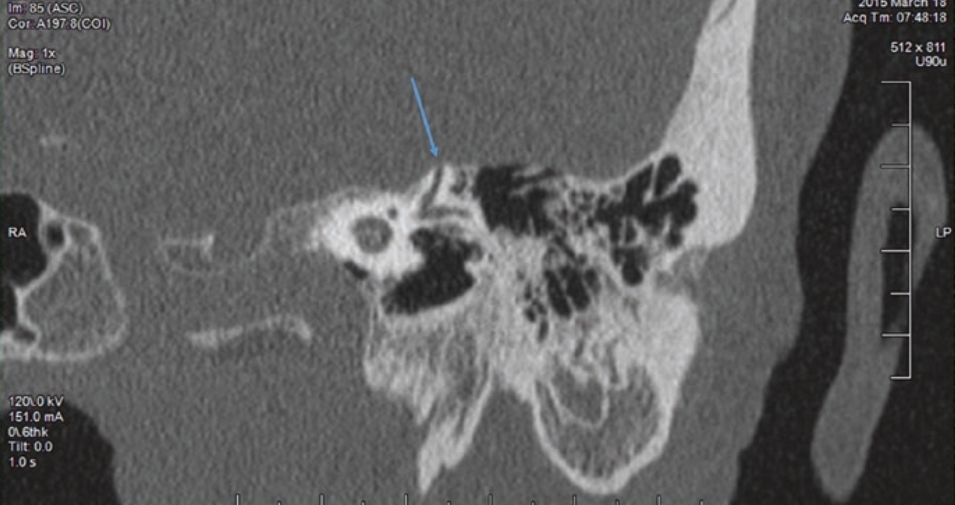
The pre-eminent example of this is superior canal dehiscence (SCD), which refers to a bony defect towards the epidural space of the superior/anterior canal.
With SCD, sound does not travel all the way up to the cochlea, but a certain amount of sound energy passes through the vestibular labyrinth, and is released through the region of the dehiscence, thereby causing vestibular symptoms mainly in the plane of the anterior canal.
SCD is frequently a radiological finding in normal, asymptomatic individuals.
Symptoms
Unspecific dizziness/unsteadiness
Brief episodes of vertigo
Tinnitus, sometimes pulsatile
Valsalva-Induced nystagmus, typically related to coughing and sneezing1
Autophony; the unusually loud hearing of a person's own voice
Signs
- Valsalva against a closed glottis will raise intracranial pressure resulting in upbeating nystagmus, with the superior pole beating towards the affected ear. This may require Frenzel lens to visualize the nystagmus.
- Sound, positive pressure in the external auditory canal, and blowing out against pinched nostrils will raise middle ear pressure resulting in downbeating nystagmus, with the superior pole of the eye directed away from the affected ear2 may be seen in patients with SCD, perilymphatic fistulas, or cranio-cervical junction anomalies, such as Chiari malformation3. This is termed Tullio’s phenomenon: sound-induced nystagmus and oscillopsia which often occurs in patients who have valsalva induced nystagmus and is commonly associated with SCD and perilymphatic fistula.
- False conductive hearing loss (since less sound is travelling to the cochlea)
- Bone conduction hyperacusis
- Hennebert sign: eye movement induced by pressure in the external auditory canal
- Ankle-Weber: tuning fork on lateral malleolus (side of stimulation is not important)
There are a number of disorders of the integrity of the bony structures of the inner ear, termed third window abnormalities, and resulting in Tullio and Hennebert signs with a low frequency air-bone gap on audiometry.
- Large vestibular aqueduct
- Cochlear dysplasia
- Vascular malformation: abnormal bony thinning between the cochlea and vascular channels
From: Magnusson M. Update in Peripheral Vestibular Disorders. J Vestib Res. Teaching Course, 29th Bárány Society Meeting, Lecture 2, June 5, 2016, Seoul, Korea.
From: https://www.youtube.com/watch?v=T9YsUVmVLPM
From: Babu, S., Schutt, C. A., & Bojrab, D. I. (Eds.). (2019). Diagnosis and Treatment of Vestibular Disorders. Springer International Publishing. https://doi.org/10.1007/978-3-319-97858-1
(vv)Tullio.mp4(tt)
Halmagyi GM. Clinical Examination of the Vestibular System. J Vestib Res. Teaching Course, 29th Bárány Society Meeting, Lecture 2, June 5, 2016, Seoul, Korea. From: https://www.youtube.com/watch?v=ehR7SOlBBow
Typically, nose pinching results in an OPEN glottis; to have the patient make a Valsalva manouevure with a CLOSED glottis, ask the patient to bear down, and to block pressure in their throat. In SCD, there is a pressure differential across the inner ear, which is connected to the spinal fluid less directly. Hence, intracranial pressure is transmitted to the superior canal via the meninges and via the perilymph of the inner ear through the cochlear aqueduct. Brief vertical and torsional nystagmus is seen which is in the plane of the superior canal.
This tecnhique does not change middle ear pressure4.
(vv)TULLIONose.mp4(tt)
From: Zee DS. The cerebellum for the neuro-ophthalmologist: A video tutorial of some signs and syndromes to recognize NANOS 42nd Annual Meeting 2016. Retrieved from: https://collections.lib.utah.edu/ark:/87278/s6nw2r5g