

Eye movement abnormalities in Wernicke’s encephalopathy include abducens nerve palsies, horizontal or vertical gaze palsies, complete ophthalmoplegia, and selective loss of function of the horizontal but not the vertical VOR1.
Gaze-evoked and upbeat nystagmus are common ocular motor findings in Wernicke’s encephalopathy, and suggest involvement of the NPH–MVN complex1. Initially there is often a spontaneous upbeating nystagmus (Video #2) that may change to downbeat nystagmus with a change in the direction of gaze, convergence or with vestibular stimuli. Vertical nystagmus in straight-ahead gaze may be markedly attenuated or reverse direction on convergence, on looking to the side, or in response to vestibular stimuli such as head shaking, applying a vibrator to the skull, or changing the position of the head relative to gravity2.
The acute upbeat nystagmus may become a chronic downbeat nystagmus.
Additional oculomotor findings include: hypometria, slow and inaccurate saccades, and impaired smooth pursuit.
Pathogenesisis
The explanation for the sparing of the vertical VOR may lie in the dichotomy that the inhibitory transmitter for the vertical VOR is GABA and that for the horizontal VOR is glycine2.
Alternatively, involvement of the NPH/MVN complex, which is located medially in the medulla and just under the area postrema, causes the bilateral, symmetric loss of the horizontal VOR and a commonly associated horizontal gaze-evoked nystagmus. More lateral structures (superior and lateral vestibular nuclei) that mediate the vertical VOR are spared, leaving the vertical VOR relatively intact.
A specific pattern of both horizontal SCC involvement is found, most likely related to enhanced vulnerability of the medial vestibular nuclei neurons because of thiamine deficiency3.

A: Aymmetric signal changes are also present in the medial thalamus (DWI);
B: Arrow points to the medial vestibular and prepostus hypoglossi nuclei (FLAIR);
C: Area of contrast enhancement in the left medial thalamus provides evidence of a disruption of the blood brain barrier during the acute phase of Wernicke's encephalopathy.
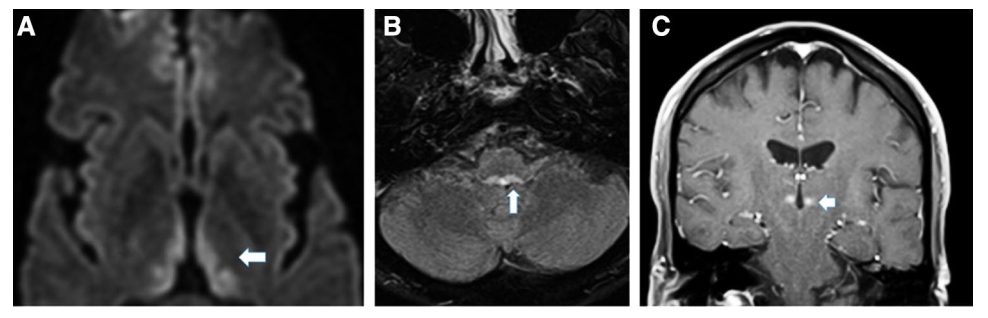
From: Kattah JC, McClelland C, Zee DS. Vertical nystagmus in Wernicke's encephalopathy: pathogenesis and role of central processing of information from the otoliths. J Neurol. 2019;266(Suppl 1):139-145. doi:10.1007/s00415-019-09326-9
(vv)Hpim 20E (Video V318) 2-18.mp4(tt)
(vv)TARNUBN.mp4(tt)
From: Dieterich M, Tarnutzer AA. Bedside ocular motor testing and vestibular testing. EAN 2020.