

Vertical saccadic gaze palsy is a characteristic features of the classic form of PSP, Richardson syndrome (PSP-RS). Patients with PSP-RS may present with visual complaints, such as blurred vision or photophobia.
The vertical gaze palsy may be detected early as loss of OKN quick phases, and at onset patients may have only slow vertical saccades without limitation of vertical gaze, one of the earliest sign of vertical supranuclear gaze palsy in PSP; determination of this requires careful examination of saccadic velocity.
Selective downgaze impairment is often believed to be representative of PSP; however, slowing of both upward and downward saccades is common and, limitation of the upward range of eye movement may be more common than downgaze limitation1.
Some patients manifest only progressive vertical gaze slowing and never progress to a limitation of the vertical range of motion in the course of their disease2. That is, a vertical supranuclear gaze palsy is not an invariable finding in PSP3.
Facial appearance and range of eye movements in progressive supranuclear palsy (PSP).
A: “Startled” facial expression attributable to facial hypomimia, frontalis overactivity, and upper eyelid retraction.
B,C: Limitation of voluntary upward (B) and downward (C) vertical gaze.
D,E: Preserved horizontal eye movements to left (D) and right (E).

From: Cordato NJ, Halliday GM, Caine D, Morris JG. Comparison of motor, cognitive, and behavioral features in progressive supranuclear palsy and Parkinson's disease. Mov Disord. 2006;21(5):632-638. doi:10.1002/mds.20779
Horizontal saccades are initially hypometric but normal in speed. With disease progression, horizontal saccades become affected and complete ophthalmoplegia may occur4. The latency of horizontal saccades may be prolonged in some patients with PSP-RS.
During vertical saccades, especially upgaze, the eyes may follow a curved rather than a linear trajectory, giving rise to so-called “round-the-house” saccades (Video 4 below). This is not specific to PSP, but is seen in any condition that leads to slowing of vertical saccades relative to horizontal saccades2.
Fixation Instability: Frequent square wave jerks are also seen to disrupt fixation..
OKN: OKN is reduced or absent in PSP, vertical more than horizontal. The eyes may appear to follow the OKN stripes, and a common scenario is for only the slow phases of OKN to be generated without any accompanying reflexive saccadic fast phase2. However, note that initially in PSP, reflexive saccades (the fast phases of OKN) are often normal.
VOR: The angular VOR is normal in PSP, but the the translational/linear VOR is markedly impaired, accounting for the impaired inability of PSP patients to converge their eyes and look at a near target.
Smooth Pursuit: Vertical smooth pursuit or combined eye-head tracking may be relatively spared5, although at higher velocities of the target, pursuit is impaired. Smooth pursuit may also be relatively impaired in PSP because it depends on neural systems involved in attention and prediction, including the parietal and frontal lobes, which are affected by tau pathology1. Eventually, SP and saccades are both lost, constituting voluntary gaze palsy
Vergence: vergence is affected early in the course of PSP, thereby accounting for the presenting complaint of horizontal diplopia in some patients1. As noted, this coexists with an impaired ability to modulate the translational/linear VOR appropriately for viewing of a near target.
Ocular abnormalities: markedly diminished blink rate, lid retraction, lid lag, blepharospam, and eye-opening apraxia are common5.
Pathogenesis
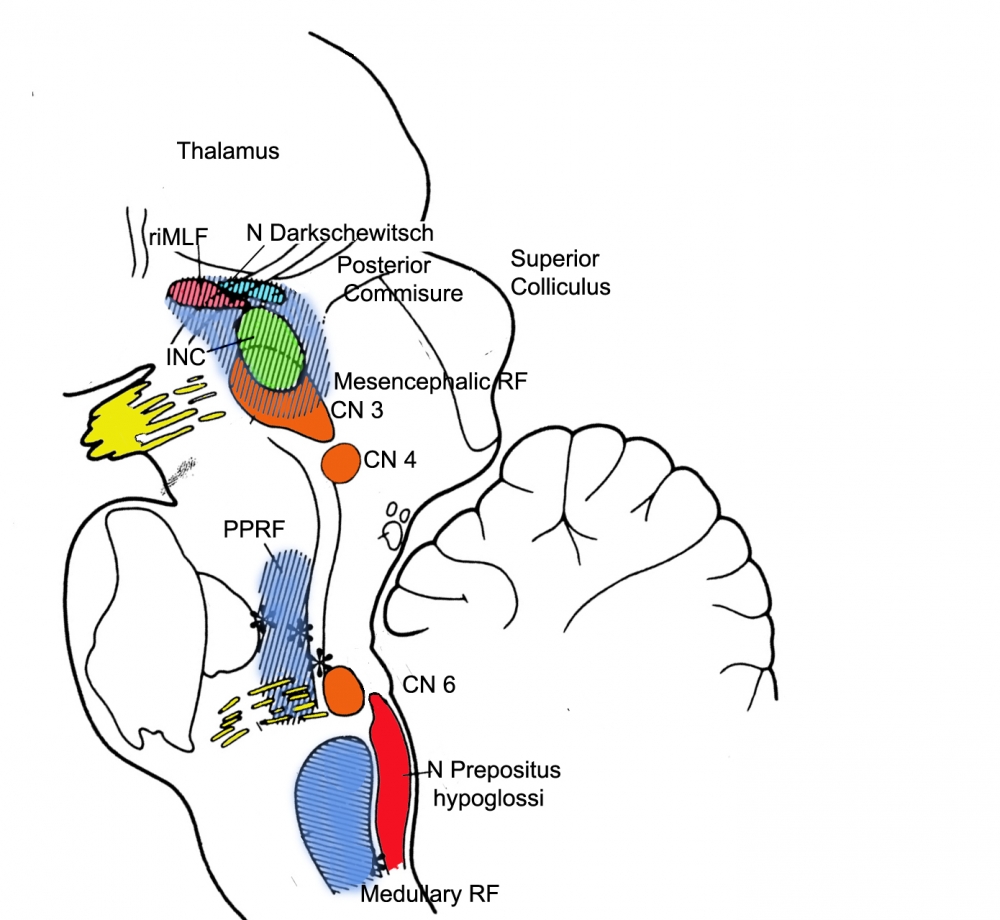
The two defects of (1) restricted range of eye movement, and (2) slowing of vertical saccades in PSP could be attributed to involvement of the INC and riMLF, respectively1. Abnormal vertical saccades result from involvement of the riMLF, brainstem reticular formation, and omnipause cells in nucleus raphe interpositus (rip)6. Vertical saccades are generated by “burst neurons” in the midbrain, and the selective involvement of vertical saccades in the early stage of PSP-RS indicates that the initial pathology involves the midbrain burst neurons, or their local circuitry (superior colliculus and the adjacent central mesencephalic reticular formation)4.
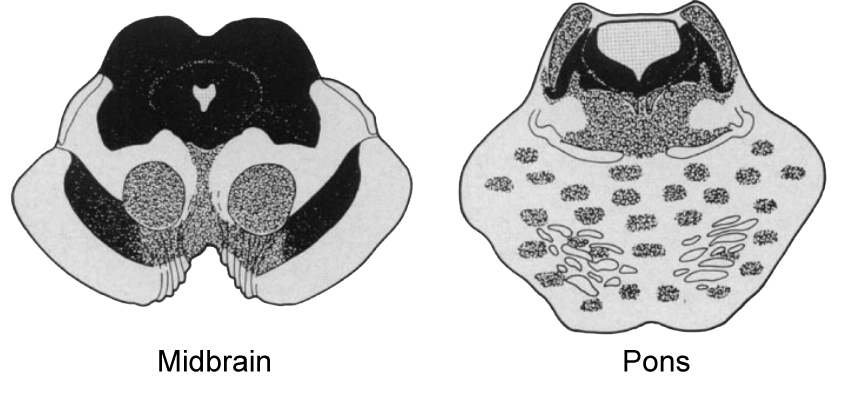
From: Steele JC, Richardson JC, Olszewski J. Progressive supranuclear palsy: a heterogeneous degeneration involving the brain stem, Basal Ganglia and cerebellum with vertical gaze and pseudobulbar palsy, nuchal dystonia and dementia. Semin Neurol. 2014;34(2):129-150. doi:10.1055/s-0034-1377058
(vv)PSP SNO.mp4(tt)
From: U-M Kellogg Eye Center in Ann Arbor. Normal and Abnormal Eye Movements. Retrieved from: https://www.youtube.com/watch?v=rRDDKKqkdTg
(vv)VORPSP.mp4(tt)
From: Termsarasab P, Thammongkolchai T, Rucker JC, Frucht SJ. The diagnostic value of saccades in movement disorder patients: a practical guide and review. J Clin Mov Disord. 2015;2:14.
This patient with PSP demonstrates frequent small-amplitude square wave jerks. When asked to keep his head still and to look up at the ceiling, upgaze saccades are slow and incomplete. When asked to look down at the floor, marked impairment of downgaze saccades is evident. Horizontal saccades are quicker, but also abnormally slowed.
(vv)PSP.mp4(tt)
From: Termsarasab P, Thammongkolchai T, Rucker JC, Frucht SJ. The diagnostic value of saccades in movement disorder patients: a practical guide and review. J Clin Mov Disord. 2015;2:14.
This patient with PSP demonstrates “round the house” saccades due to a vertical supranuclear gaze defect. Horizontal saccades are relatively preserved. Pursuits are relatively normal, though vertical range remains impaired.
(vv)2PSP.mp4(tt)
From: Termsarasab P, Thammongkolchai T, Rucker JC, Frucht SJ. The diagnostic value of saccades in movement disorder patients: a practical guide and review. J Clin Mov Disord. 2015;2:14.