

Midbrain structures are especially important for the control of vertical eye movements, including saccades and gaze-holding. Midbrain lesions can result in a vertical gaze palsy and vertical nystagmus due to impaired vertical gaze-holding.
The critical structures for vertical eye movements include the:
- Rostral interstitial nucleus of the medial longitudinal fasciculus (riMLF)
- Interstitial nucleus of Cajal (INC)
Limitation of conjugate upgaze occurs with damage to the pretectum, an isthmus between the superior colliculi and the thalamus. Supranuclear fibres which control vertical gaze (upgaze greater than downgaze) decussate through the pretectum (posterior commissure) as they pass to the riMLF,
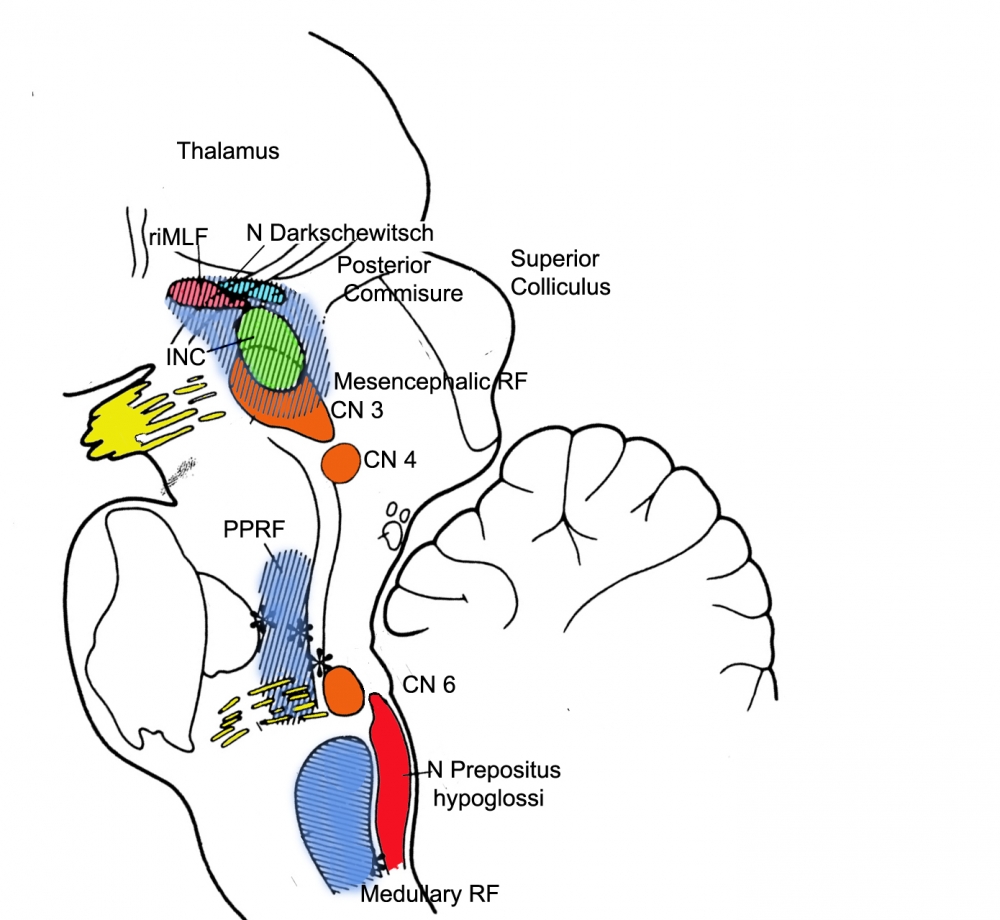

- Lesions of the riMLF result in a saccadic gaze palsy. The riMLF is involved in generating vertical saccades, and the quick phases of vertical nystagmus (and thus is the homologue of the PPRF for horizontal saccades). The riMLF also produces the quick phases of torsional nystagmus during rotation of the head in the roll plane (lateral tilt). Each riMLF contributes to both upward and downward saccades, but each generates torsional quick phases in just one direction; for example, the right riMLF is responsible for the quick phases to the right side, with extorsion of the right eye and intorsion of the left eye.
Bilateral lesions of the riMLF, as in artery of Percheron infarction, will cause loss of downward or all vertical saccades and abolish all torsional quick phases2. A unilateral lesion abolishes ipsilesional torsional quick phases2. - The INC plays a key role in holding eccentric vertical gaze. The INC projects to the ocular motoneurons, mainly via the posterior commissure. For vertical saccades, this projection is to yoked muscle pairs (eg, the inferior rectus and superior oblique muscles for downward saccades)2.
Lesions of the INC produce an ocular tilt reaction and, in contrast to the lesions of the riMLF, cause ipsitorsional nystagmus with quick phases moving the top poles of the eyes toward the side of the lesion
Saccades
Saccadic gaze palsy (SGP) is associated with slowing of saccades vertically or horizontally (or both), with or without range limitations2. Saccade slowing in isolation is evidence of SGP, even if the range of eye movement is full.
Loss of quick phases of optokinetic nystagmus are likely to be an early feature of a supranuclear gaze palsy2.
It is important to note that isolated mildly impaired eye elevation is not sufficient to diagnose SGP, since this may be seen in healthy elderly individuals2.
Note that, in addition to midbrain lesions, saccadic slowing may arise from dysfunction of the cerebral hemispheres, superior colliculus, and cerebellum2.
Causes of Vertical SGP:
- Artery of Percheron infarction. The terminal supply is to the pretectum, and ischaemia in the artery's territory may infarct the riMLF, resulting in vertical saccadic gaze deɹcits with relative sparing of vertical pursuit and vestibular-ocular movements.
- Following cardiac surgery
- Progressive supranuclear gaze palsy (PSP), corticobasal generation and frontotemporal dementia
- Niemann-Pick type C (NP-C). This autosomal recessive disorder is characterized by deposition of sphingolipid, which affects the midbrain and riMLF
Vertical saccade paresis may be present before the neurological or psychiatric manifestation and is sometimes the only symptom of NP-C in adults. Initially, slow vertical saccades, especially downwards, often accompanied by horizontal oscillations (as an expression of activation of the intact horizontal saccade system) and frequent blinking occur3. Since horizontal saccades may lie be normal, when patients make diagonal saccades, the trajectories of these movements are strongly curved4.
Vertical optokinetic nystagmus, as tested by an optokinetic drum, is often absent (as occurs in PSP). As the disease progresses, complete vertical gaze palsy with the inability to look upward or downward occurs. The VOR is often preserved until very late, indicating that the gaze palsy is truly supranuclear in nature. - Paraneoplastic: anti-Ma2 encephalitis
- Anti-GAD antibody syndromes are associated with slow vertical saccades
- Glycine receptor antibody-positive progressive encephalomyelitis with rigidity and myoclonus: slowing of upward saccades
- Creutzfeldt–Jakob disease (sporadic and familial)
- Whipple's disease
Smooth Pursuit and VOR
Vertical smooth pursuit and the vertical VOR may be involved if the MLF projections are affected as they pass through the midbrain. Bilateral lesions of the riMLF are common, due to their supply being from a single perforating vessel (the artery of Percheron). These lesions may cause loss of downward, or all vertical saccades, as well as torsional quick phases of nystagmus.
See also: Parinaud's syndrome