Cervical dystonia (CD) is a form of focal dystonia in the neck muscles, and is also called torticollis.
A wide variety of abnormal positions of the head and neck can be present, and there is often a mixed picture. Cervical muscles are said to have a redundant organization, meaning that each head and neck movement can be generated by more than one muscle or muscle combinations. Unfortunately, phenomenology alone is frequently insufficient to determine the most appropriate muscle for injection.
COL-CAP concept Examination/& Muscle Selection Anatomy of Cervical Dystonia Ultrasound of Cervical Dystonia
The main forms of CD are:
|
|
|

Muscle Selection
About a third of patients with CD are reported to have a poor response to botulinum toxin injections. In part, the reason for this may be an oversimplistic approach, assuming that CD predominantly affects the superficial muscles of the neck. Superficial muscles (Splenius, Sternocleidomastoid, Trapezius) are easy to inject but are not universally responsible for the abnormalities of head posture. Certain patients may have dystonia of deep muscles, such as obliquus capitis inferior (OCI), longissimus capitis, and the scalene muscles. There are multiple neck muscles with overlapping functions, which may generate the same movement, although different combinations of muscles are involved. The commonest reason for failure of botulinum toxin treatment is that the correct muscles have not been identified, or that accurate injection of a desired muscle has not been achieved.
A critical question in CD is the site of action of the dystonic muscles: primarily related to muscle attachment to the skull, or to the neck. As an example, the sternocleidomastoid muscle, inserted on the mastoid process, is only able to act on the head, and the semispinalis cervicis muscle, inserted on the cervico-thoracic spine, can only exercise action on the neck. Distinguishing between caput and collis has improved results as measured by the TWSTRS2.
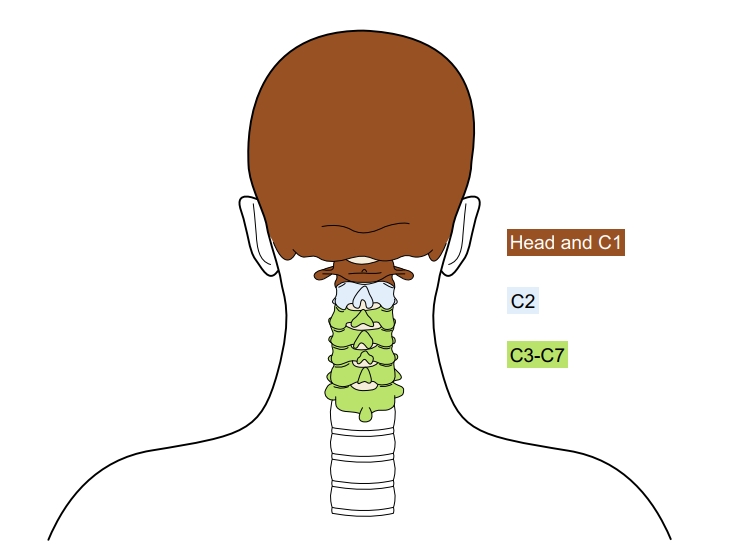
The C2/C3 vertebra can be regarded as a fixed point. This is related to the numerous muscles which insert at the spinous process of C2 (obliquus capitis inferior, rectus capitis major, semispinalis cervicis, multifidus)3.

Computed tomography has shown that approximately half of the neck rotation occurs at the C1-C2 (atlanto-axial) level, centred around the odontoid process:

The 2nd commonest region for rotation is the midcervical region (approximately 5 degrees), and the C7-T1 segment the least.
There is virtually no rotation occurring between occiput and atlas: the ellipsoid form of the atlanto-axial joints allows for flexion-extension, and to a lesser extent, for lateroflexion4.
Given the importance of the axis (C2 vertebra) in CD, dystonia affecting the head and neck muscles can be divided into two groups, caput (head) and collis (neck):
- CAPUT: The upper level group of muscles acts at the head and C1 (the atlas); this is dystonia of muscles acting on the joints of the head at the atlanto-occipital joints (laterocaput/torticaput)3.
- COLLIS: The lower level group of muscles acts at C3-C7; this is dystonia of muscles acting on the cervical spine (laterocollis/torticollis).
- The two levels are able to move independently, the upper level in relation to the lower one, and the lower level in relation to the thoracic spine.
- Varying degrees of caput- and collis- involvement are seen. In lateral, forward and backward flexion, a clinical determination of the dominant group (caput or coll) is usually accurate. However, in patients with rotation of the neck, clinical assessment may be inaccurate5.
-
Noting that most patients have two or more subtypes, the commonest form of CD is torticaput, followed by laterocaput6. Laterocollis and torticollis are seen in less than 10% of patients7.
Muscles may also be divided on the basis of their function, and relationship to how the abnormal head posture is produced:
- Dystonic muscles are able to induce abnormal movement, posture or spasms. They will be abnormally active on EMG, and are the principal target of botulinum toxin therapy.
- Antagonist muscles are passively tensed as a result of abnormal movement or posture; passive stretch may result in pain 8. They can sometimes act as true antagonist muscles resulting in movement that is in the opposite direction to the dystonic activity, or may cause tremor. In rare cases, they should also be injected.
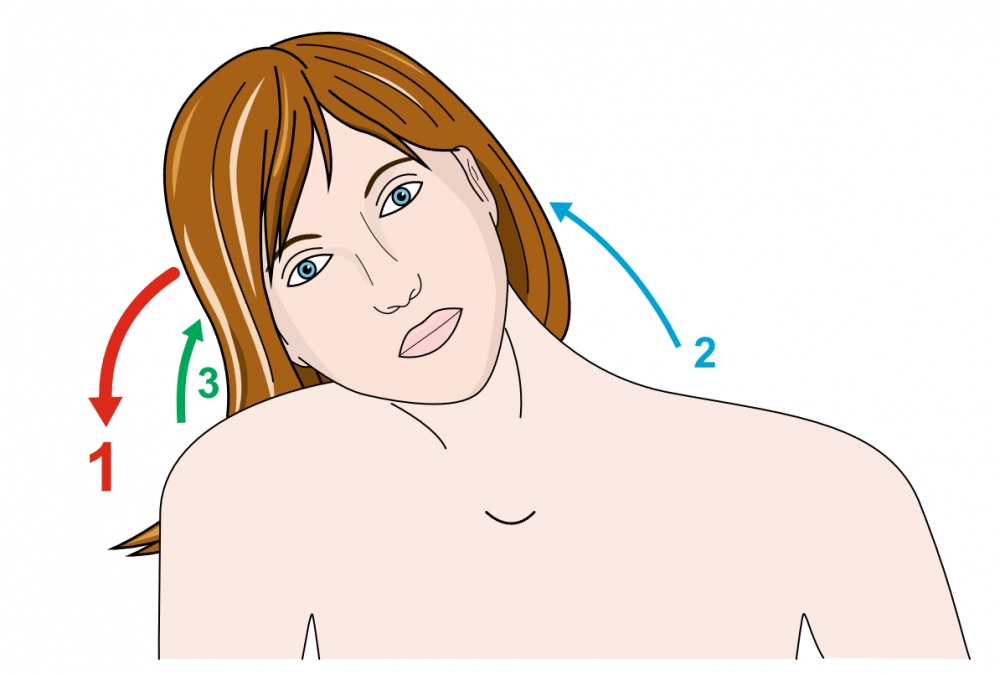
- Compensatory muscles may help patients to correct their posture and gaze. This compensation is useful for patients, and these muscles should not be treated with botulinum toxin. In addition, compensation can mask an abnormal movement. For example, shoulder elevation can limit lateroflexion of the head and neck. During clinical examination, when the shoulder is fixed, the abnormal movement will become more obvious (Figure 2).

From: Reichel G. Cervical dystonia: A new phenomenological classification for botulinum toxin therapy. Basal Ganglia 2011; 1: 5–12.
Note that the col-cap approach is used for dystonic postures, but not for the fast or jerky component that contributes to dystonic movements.
 |
Example of right lateroflexion: 1. Right paravertebral muscles (splenius, semispinalis) are dystonic. 2. Left trapezius is antagonistic, passively tensed by abnormal movement. 3. Right Levator scapulae is compensatory.
|
From: Tatu L, Jost WH. Anatomy and cervical dystonia: “Dysfunction follows form”. J Neural Transm 2017; 124: 237–43.

From: Reichel G. Dystonias of the Neck: Clinico-Radiologic Correlations. In: Dystonia - The Many Facets. InTech, 2012. DOI:10.5772/27896.
Note relationship of surface markings:
1. Sternal notch and Larynx: deviated from one another in the case of torticollis, but not torticaput.
2. The relationship of the external auditory meatus to the clavicle. In the case of ante- and retrocollis, the meatus is displaced anteriorly or posteriorly. In the case of caput conditions, the meatus lies over the clavicle.

From: Tatu L, Jost WH. Anatomy and cervical dystonia: “Dysfunction follows form”. J Neural Transm 2017; 124: 237–43.
Features on history which may help with identifying muscle selection:
- Which form of deviation of the head causes the most disability?
- Which movements are difficult to perform?
- Which muscles are painful?
Examination features for muscle selection:
Ideally the patient is seated parallel to the observer on a chair without a backrest. Note that deep muscles are not accessible, whereas superficial layers may be both inspected and palpated, and muscles in the intermedite layer may be palpated.
Inspection |
|
Palpation |
|
Examination protocol |
|
EMG
EMG is useful for identifying muscles which are dystonic, and for ensuring that the toxin is delivered to the correct muscle. An important issue is that abnormal neck positions may be caused by different combinations of dystonic activity, and that this may only be resolved with EMG. A particular issue with use of EMG is the difficulty of distinguishing a dystonic muscle from one which is compensatory.
Alternative approaches might be to use ultrasound or MRI to assess muscle hypertrophy.
- Use of a Rating Scale may be of value.
- Videotaping may be of value for comparison subsequently with the initial presentation.
Major Side Effects of injecting botulinum toxin for CD
Note that adverse events decline after initial treatment sessions11,12. It appears likely that the degree of spread from the site of injection to adjacent muscles may vary depending on the product used.
- Swallowing difficulties. The highest risk of swallowing difficult arises from injection of the lower third of the sternocleidomastoid muscle, especially if bilateral.
- Weakness of neck extensors is also a common side effect, typically associated with injections of semispinalis capitis.
The spectrum of involuntary movements or abnormal postures of the head and neck is very varied with respect to speed, amplitude, rhythmicity, duration and direction of movements. Smaller amplitude, higher frequency movements may be superimposed on the large amplitude movements. These may be horizontal, vertical or mixed tremulous oscillations.
Patients typically belong to one of the following groups:

| PHENOMENOLOGY | Posture dominant subtype: few dystonic movements (which mainly occur with voluntary head repositioning) | Tremor Dominant subtype |
|
(vv)MDS3.mp4(tt) Inspection: Left sternocleidomastoid hypertrophic and hyperactive Prevalent phenotype: Head rotation towards the right, mild tilt to the left Dystonic Postures: present Dystonic Movements: none Active Range of Head Motion: to left and right Pain: none
|
(vv)MDS4.mp4(tt) Prevalent phenotype: Tremulous, mainly NO-NO phenotype; jerky component varying in frequency and direction Dystonic Postures: A sagittal shift with mild retrocollis Dystonic Movements: Variable head tremor: - At rest with open eyes - Disappearing with closed eyes - Attenuating with head rotation to either side - Increasing with walking or raising arms Active Range of Head Motion: limited bilaterally |
|
| Muscle Selection |
|
|
| PHENOMENOLOGY | Mobile Postural subtype | Jerky and Postural Subtype: evenly weighted degree of postures and movements |
|
(vv)MDS1.mp4(tt) Prevalent phenotype: a variety of mobile postures (slow or fast), with some tremor. Dystonic Postures: Left head rotation and right head tilt Dystonic Movements: Occasional left head tilt and left shoulder elevation (requires verification by instrumented assessment) Active Range of Head Motion: Limited, particularly to the right. |
(vv)MDS2.mp4(tt) Prevalent phenotype: Segmental dystonia with cranial and cervical involvement. Dystonic Movements: Predominantly jerks at rest with eyes closed and when attempting to turn her head to the right. Diminishing jerky movements and predominant postures with complete head rotation to the right. |
|
| Muscle Selection |
|
|
Further examples:
Rotation of head to the right
|
Muscles injected: |
(vv)CD Short.mp4(tt)
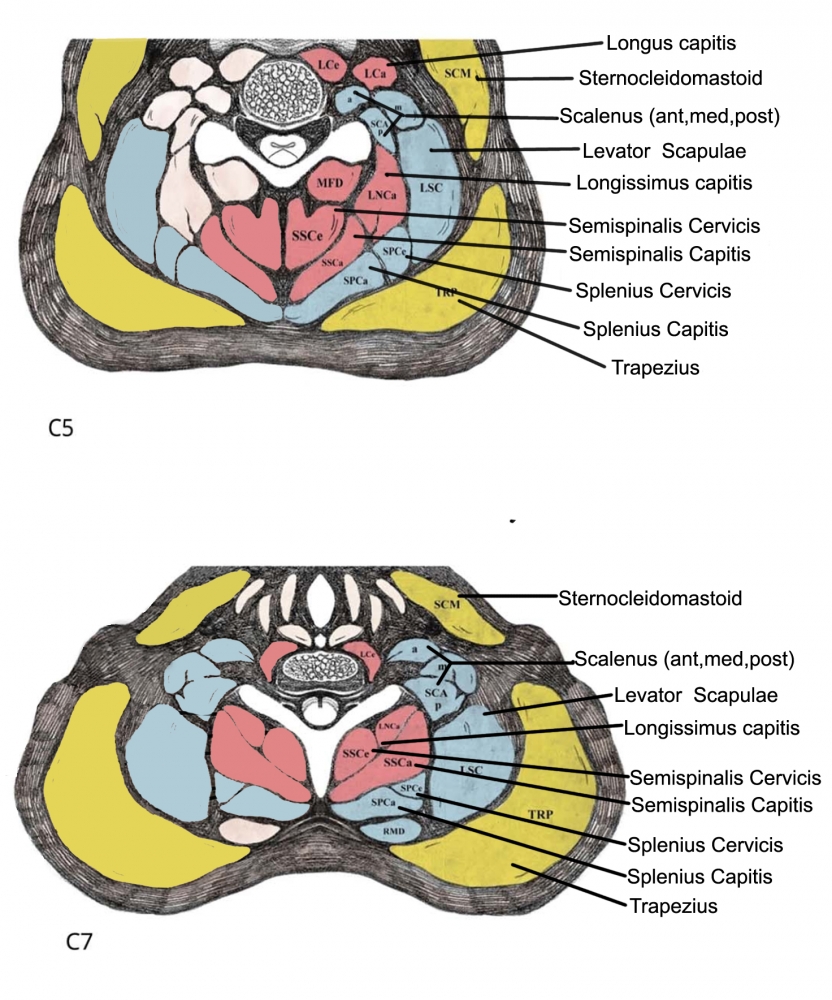
A. The posterior triangle of the neck is delineated by the posterior edge of the sternocleidomastoid muscle and the anterior edge of the trapezius muscle. The base of the triangle is the middle third of the clavicula, and the apex of the triangle, behind the mastoid process, is a narrow area where sternocleidomastoid and trapezius muscles meet.
The following muscles are found in the triangle, and synergy of action is found in these muscles, due to identical muscle fibre orientation:
Sternocleidomastoid + Trapezius
Splenius + Levator scapulae
B. The important flexor muscles of the neck (longus colli and longus capitis) are shown:
| A | B |
 |
 |

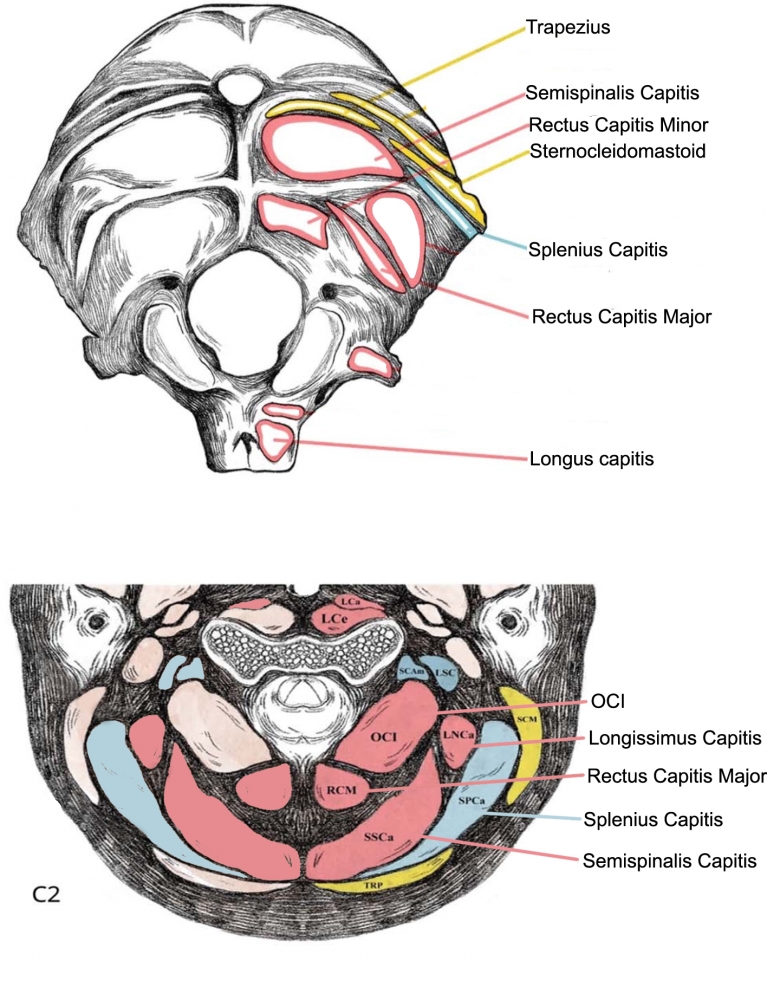
Suboccipital deep muscles lie deep to splenius capitis, and are mainly responsible for extension and rotation.
The anterior deep muscles flex the neck and head.
|
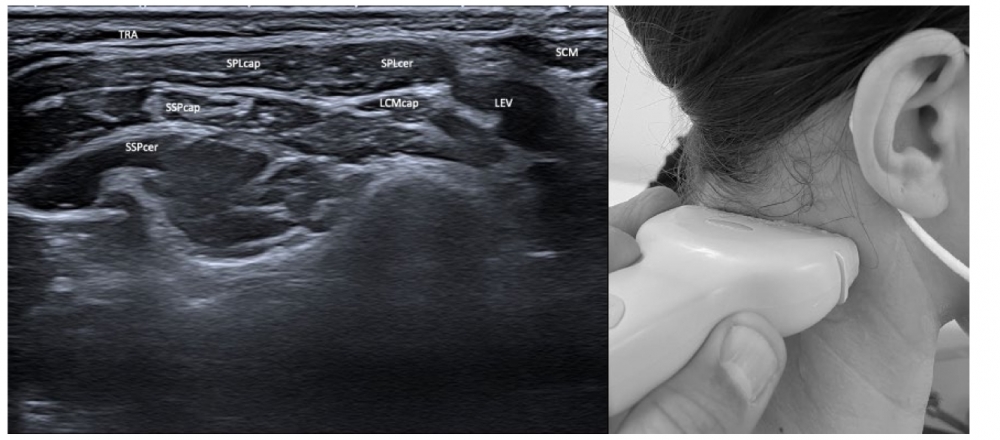
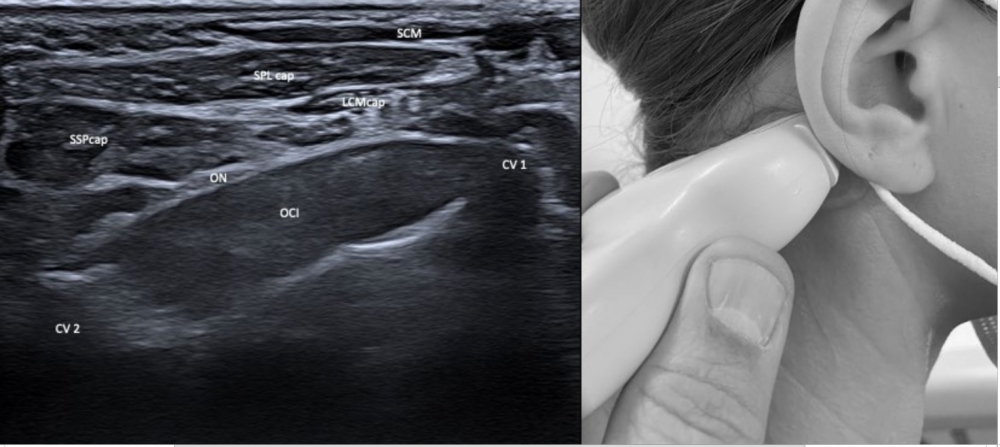
ULTRASOUND OF CERVICAL DYSTONIA Superficial Layers: TRA: Trapezius
Deep Layers SCM: Sternocleidomastoid CV1 & 2: Atlas and axis vertebrae
|
LATERAL
POSTERIOR Superficial
Intermediate
Deep
|
|