

From: Reichel G, Stenner A, Janh A. [Cervical dystonia: clinical-radiological correlations and recommendations for the correction of botulinum therapy]. Zh Nevrol Psikhiatr Im S S Korsakova. 2012;112(1):73-9. Russian. PMID: 22678680.
Head rotation often occurs together with neck rotation. It is classically caused by activation of the ipsilateral splenius capitis, the contralateral sternocleidomastoid muscle and the ipsilateral trapezius/semispinalis capitis muscle complex. However, deep posterior neck muscles arising from the atlas and the axis including the obliquus capitis inferior, the rectus capitis posterior major and the rectus capitis posterior minor muscles are strong ipsilateral head rotators. The levator scapulae muscle is an additional but weaker ipsilateral head rotator. In head and neck rotation, the role of the sternocleidomastoid is often overestimated, whereas the role of the splenius capitis and the deep posterior neck muscles is often underestimated1.
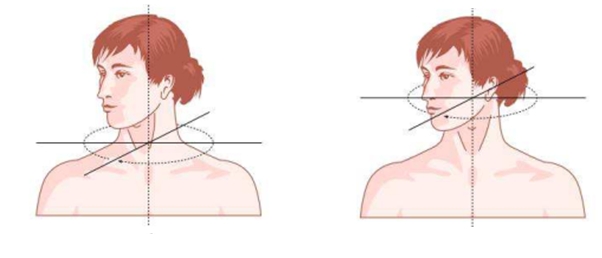
Two levels of movement take place:
Torticollis
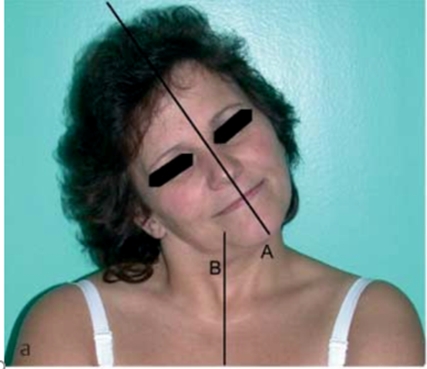
When rotation takes place at the lower level of the cervical spine, between C2 and C7, rotation of the neck takes place in relation to the trunk (torticollis). In torticollis, the larynx/Adam’s apple rotates laterally, and the head is also rotated due to the rotation of the neck.
Torticaput
When rotation takes place at the upper level of the cervical spine, between the skull and C2/C3, where muscles act at the atlanto-occipital joints, the head rotates and the neck remains in a vertical/upright position, leading to a torticaput.
In torticaput, the Adam’s apple is found largely in a medial position.
Distinguishing torticollis and torticaput
Distinguishing between torticollis and torticaput may be clinically difficult to achieve, and additional tests may be required, such as CT or MRI of the cervical spine. In general, an analysis of the position of the sternal notch with relationshin to the larynx is helpful. Should the diagnosis remain unclear, CT sections at the C1-C3 level and the C7 plane may be obtained. By comparing the position of the vertebra in both planes, torticollis and torticaput can be distinguished from one another. .

- Splenius may act with levator scapulae: shoulder elevation on the side to which the neck is rotated suggests dystonic levator scapulae.
- Trapezius may act with SCM: shoulder elevation on the opposite side to the direction of rotation suggests dystonic trapezius.

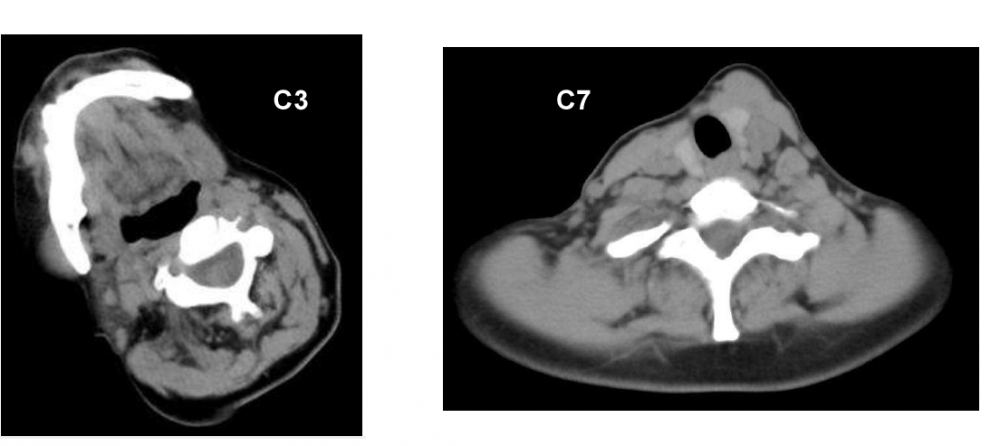
Torticollis
CT at levels C3 and C7 (note the C3 level is identified by the mandible being visible on the image)
At C3 the cervical vertebrum is in line with the skull, and away from C7
|
|
|

- Head rotation is towards the right, mild head tilt to the left
- Left sternocleidomastoid: hypertrophic and hyperactive
(vv)MDS3.mp4(tt)
The mark over the superior thyroid notch is rotated in relation to the mark over the jugular notch of the manubrium sterni.
CT scan in this patient with torticollis shows that C1 and C2 are rotated, whereas C7 is straight. Rotation therefore occurs between C3 and C7; only muscles acting on the cervical spine are affected.

From: Reichel G. Cervical dystonia: A new phenomenological classification for botulinum toxin therapy. Basal Ganglia 2011; 1: 5–12.
TREATMENT
In rotational CD, the classical approach is injecting the ipsilateral splenius capitis and the contralateral sternocleidomastoid. However, this is largely a treatment for torticaput (note that sternocleidomastoid inserts into the mastoid process, and therefore cannot cause torticollis).
Alternative scheme and muscles for injection shown: (After: Jost WH, Tatu L. Selection of Muscles for Botulinum Toxin Injections in Cervical Dystonia. Mov Disord Clin Pract 2015;2(3):224–6)
- Semispinalis cervicis
- Levator scapulae
- Splenius cervicis (secondary)
- Longissimus cervicis (secondary)
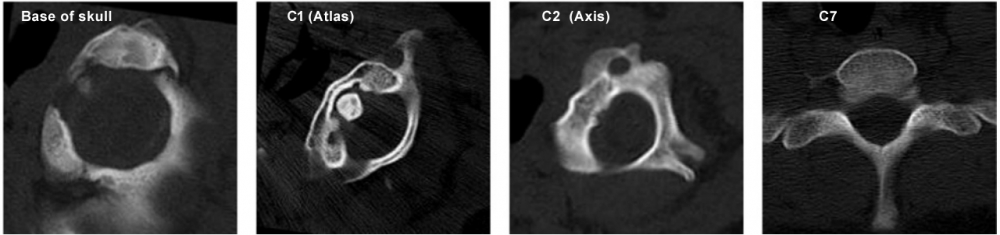
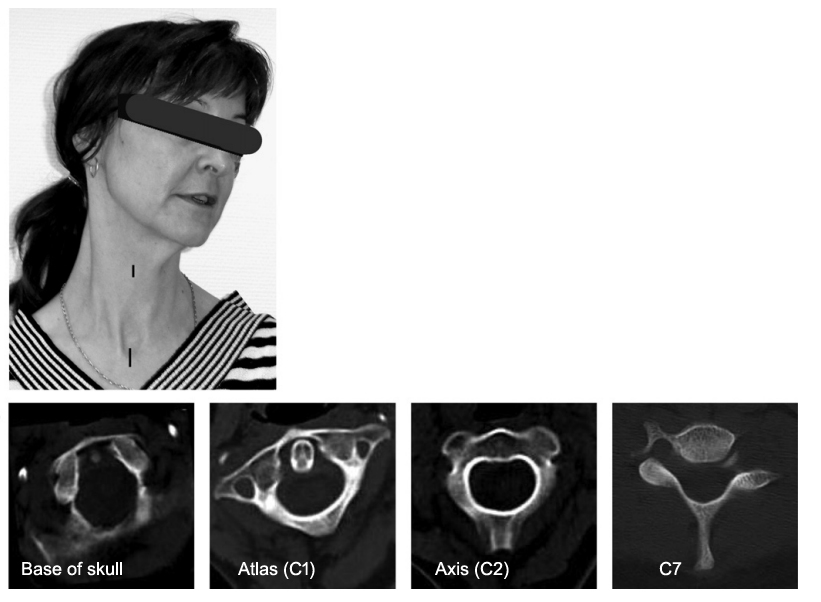
Torticaput
Imaging demonstrates that the base of the skull and 1st cervical vertebra are rotated whereas C2 and C7 are straight.
The rotation occurs between C1 and C2 (the atlanto–axial joint); consequently only the muscles acting on the skull are involved in causing the torticaput.
From: Reichel G. Cervical dystonia: A new phenomenological classification for botulinum toxin therapy. Basal Ganglia 2011; 1: 5–12.
From: Reichel G, Stenner A, Jahn A. The phenomenology of cervical dystonia. Fortschr Neurol Psychiatr 2009; 77: 272–7.
TREATMENT (After: Jost WH, Tatu L. Selection of Muscles for Botulinum Toxin Injections in Cervical Dystonia. Mov Disord Clin Pract 2015;2(3):224–6)
Contralateral to side of rotation
1. Trapezius (Descending portion)
3. Semispinalis capitis (secondary)
Ipsilateral to side of rotation
4. Obliquus capitis inferior (main)
5. Longissimus capitis (secondary)
6. Splenius capitis (secondary)
Obliquus capitis superior may also be injected