

Retrocollis Retrocaput Backward Sagittal Shift
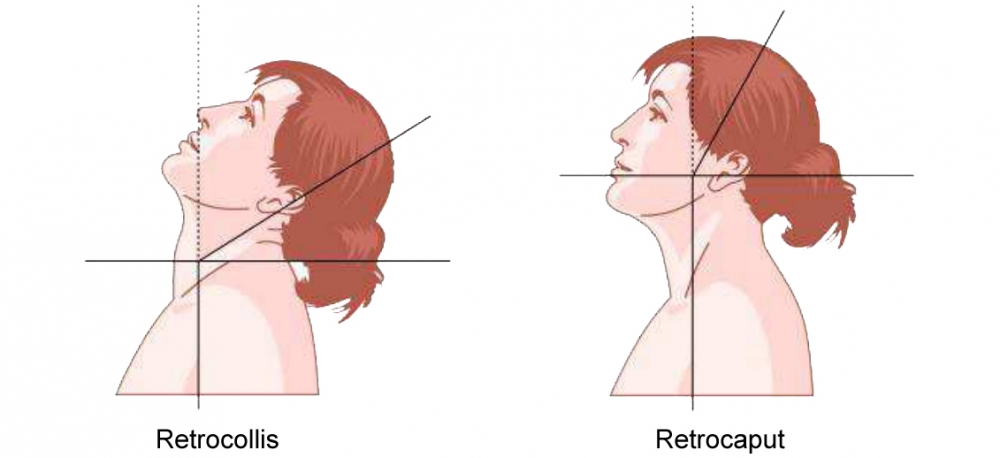
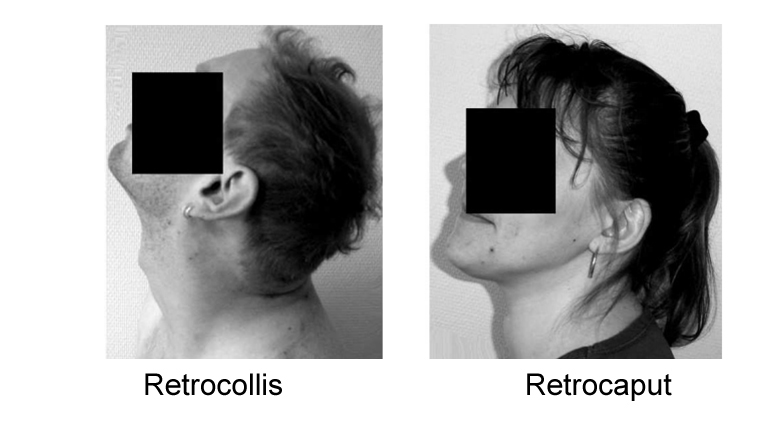
Retrocollis
The neck is tilted backwards in relation to the thoracic spine; the angle between the neck and head is normal1
Retrocaput
The head is tilted backwards at an angle on the neck; the angle between the cervical and thoracic spine is normal1.
Distinguishing retrocaput and and retrocollis
Analysis of backward flexion (differentiation between retrocollis and retrocaput) can be accomplished by observation from the side of the respective angles between the cervical and thoracic spine (retrocollis), and between the cervical spine and the base of skull (retrocaput)2.
In cases of severe retrocollis, it is difficult, in practice, to distinguish the extension of the cervical spine (hyperlordosis) from the extension of the head on cervical spine. In that case, it may be more important to choose a high dose of botulinum toxin and an appropriate needle for deeper injection rather than to try to distinguish each muscle of the posterior cervical region during the injections as all the posterior cervical muscles can be involved in the extension3.
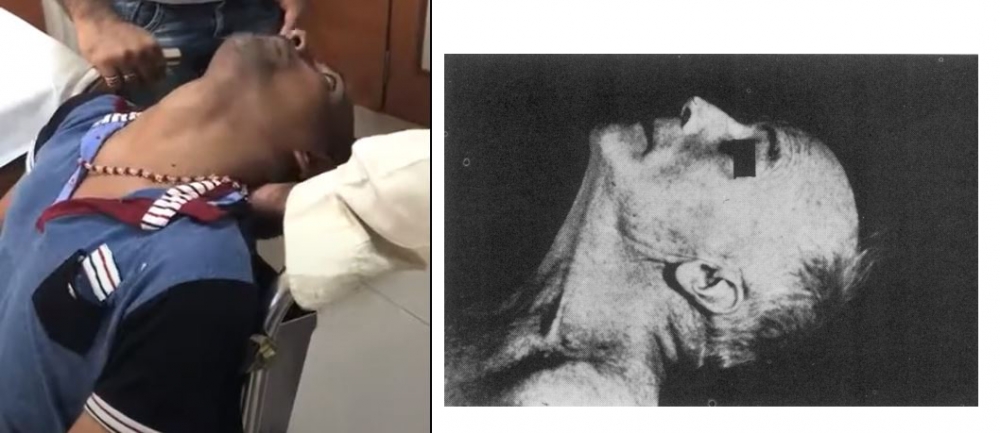
From: Srinivasan,S. (2019, August,2). Severe retrocollis with trunk dystonia (Video). YouTube. https://www.youtube.com/watch?v=5-tv9pkQ7TA and Cooper IS. Effect of Thalamic Lesions upon Torticollis. N Engl J Med 1964; 270: 967–72.
RETROCOLLIS
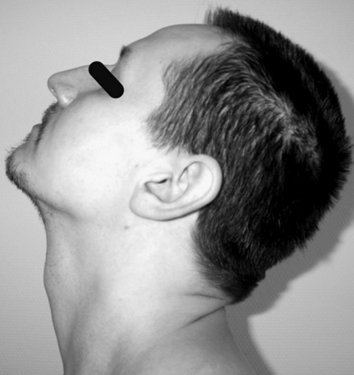
From: Reichel G. Cervical dystonia: A new phenomenological classification for botulinum toxin therapy. Basal Ganglia [Internet] 2011;1(1):5–12.
TREATMENT
Semispinalis Capitis 2 x 7.5 u; Max 50 u Botox;2 x 30-40; Max 200 u Dysport
And/or splenius capitis Bilateral 2 x 10-12.5 u; Max 20 u Botox; 2 x 40-50; Max 2 x 80 u Dysport
Alternative scheme: Bilateral Semispinalis Cervicis (After: Jost WH, Tatu L. Selection of Muscles for Botulinum Toxin Injections in Cervical Dystonia. Mov Disord Clin Pract 2015;2(3):224–6):

From: Reichel G. Cervical dystonia: A new phenomenological classification for botulinum toxin therapy. Basal Ganglia [Internet] 2011;1(1):5–12.
TREATMENT
Bilateral (After: Jost WH, Tatu L. Selection of Muscles for Botulinum Toxin Injections in Cervical Dystonia. Mov Disord Clin Pract 2015;2(3):224–6)
1. Obliquus Capitis Inferior
2. Semispinalis Capitis
3. Trapezius (pars descendens)
4. Splenius Capitis
Additional Muscles to consider:
Rectus capitis major
Obliquus capitis superior
Longissimus capitis
Sternocleidomastoid