

The muscles involved in opening the jaw are:
- Inferior head of the lateral pterygoid. This is typically the primary muscle involved.
- Submental complex (which includes the digastrics, mylohyoid, and geniohyoid muscles). The complex has a secondary role in promoting jaw opening, primarily assisting jaw opening at the start of the movement.
Anatomy
The lateral pterygoid muscle has superior and inferior heads. Involvement of the inferior head is the usual cause of jaw opening dystonia, and for practical purposes, the superior head is not typically injected.
- The superior head arises from the greater wing of the sphenoid (infratemporal surface) and inserts into the capsule of the tempero-mandibular joint.
- The inferior head arises from the outer surface of the lateral pterygoid plate and inserts into the condylar process of the mandible. (note that the medial pterygoid muscle arises from the medial surface of the lateral pterygoid plate)
Action:
The two heads have separate, reciprocal functions: when the inferior head contracts, the superior head of the pterygoid muscle is inhibited.
When the inferior head of the muscle is activated unilaterally, a contralateral deviation of the jaw is produced, usually in concert with the medial pterygoids.
Conversely, during jaw closure, the superior head contracts, and the inferior head relaxes. The superior head acts to stabilize the condyle during jaw closure.
When acting bilaterally, the inferior head of the pterygoid muscle pulls the condyle forward and slightly downwards, and produces jaw protrusion and jaw opening (acting in conjunction with the suprahyoid muscles).
 |
 |
From: Blitzer, A., Benson, B. E., & Guss, J. (2012). Botulinum Neurotoxin for Head and Neck Disorders. Thieme Medical.
 |
 |
TREATMENT
Injection of the inferior head of lateral pterygoid. There are two approaches, external and intraoral.
1. External injection
The examiner should palpate for the mandibular notch (the gap between the coronoid process anteriorly and the mandibular condyle posteriorly), which is found immediately beneath the zygomatic arch. This is easily felt as the patient opens and closes their jaw. The needle is passed horizontally through the notch into the lateral pterygoid, which is activated by jaw opening, typically with EMG guidance.
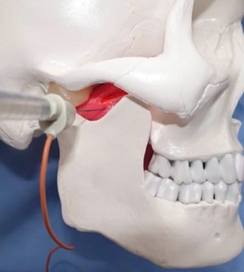
Potential side-effects: The maxillary artery is relatively superficial and is therefore potentially prone to trauma from the injecting needle, potentially resulting in haematoma formation.

2. Intraoral injection
The muscle may be injected intraorally, also with EMG guidance. This allows for placement of toxin to a wider part of the muscle.
In the intraoral injection, the patient should be semi-reclined with their mouth slightly open and deviated contralaterally to the side of the procedure.
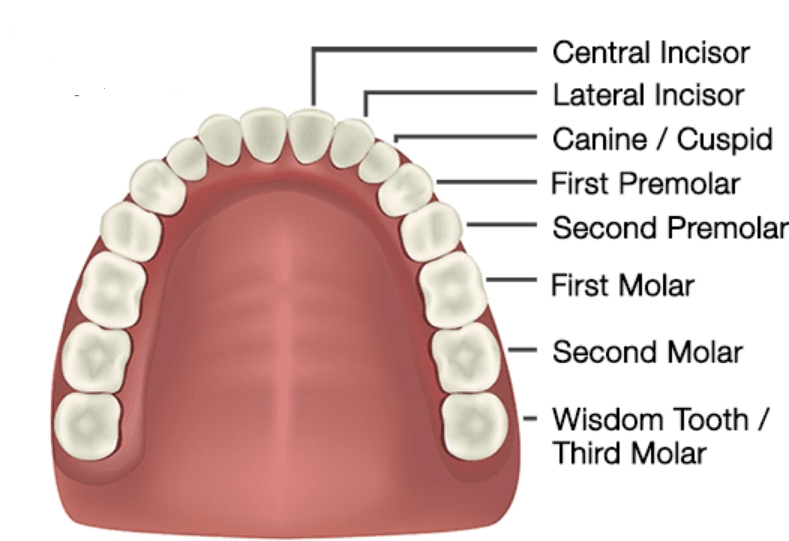
The insertion of the needle electrode to inject the inferior head is above the second molar mucobuccal fold (the fold formed by the oral mucosa where it passes from the maxilla to the cheek). The electrode is directed medially (by 200), upward (by 300 to the occlusal plane (the plane formed by opposition of the teeth of the upper and lower jaw), and backward sliding close to the maxillary tuberosity (the bump felt at the back fo the maxilla, related to the wisdom tooth) until hitting the pterygoid plate.The direction of the injection should be oriented towards the middle point of a virtual line connecting the ipsilateral ear’s tragus and lobe.

The needle must penetrate (at least 30–40 mm) through the masseter muscle and temporalis tendon before reaching the inferior lateral pterygoid head.
Once the needle is in position, the patient is asked to produce lateral excursions of the jaw to confirm proper placement.

From: Yoshida K. How Do I Inject Botulinum Toxin Into the Lateral and Medial Pterygoid Muscles? Mov Disord Clin Pract. 2016 Dec 14;4(2):285. doi: 10.1002/mdc3.12460.
Dose
7.5 u Botox
(vv)Lay Pty.mp4 (tt)