

-
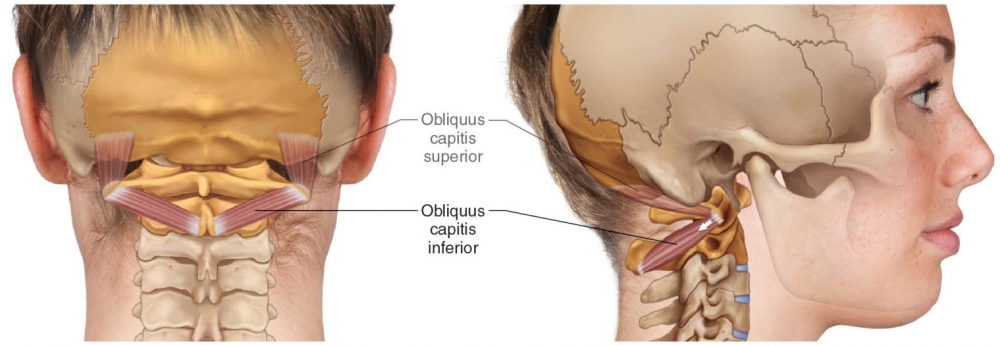
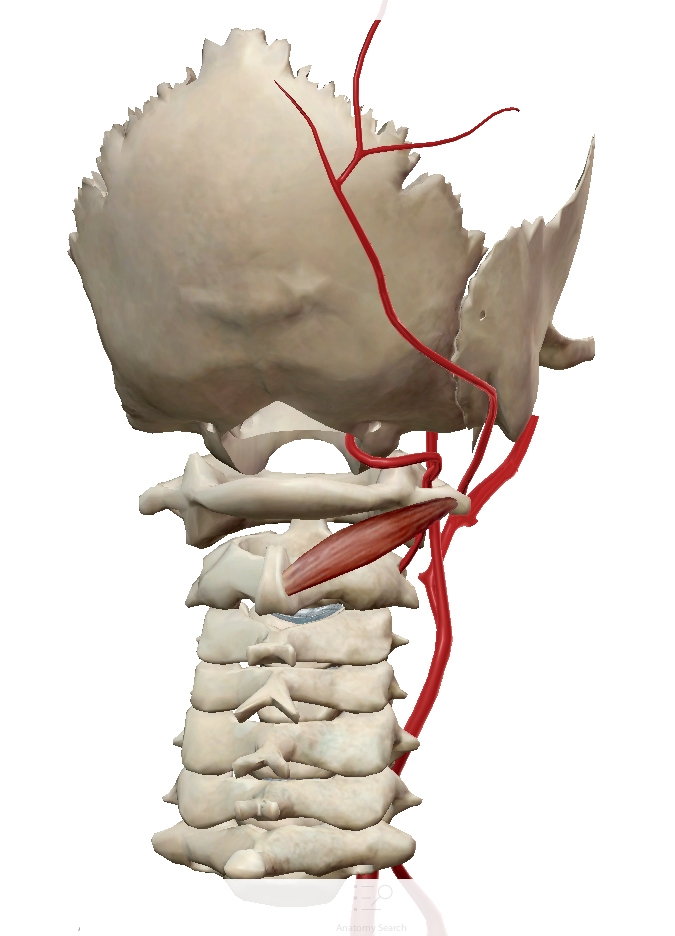
Origin: posterior spinous process and adjacent lamina of axis.
-
Insertion: transverse process of atlas
-
Action: rotates atlas upon axis, thereby rotating head to same side.
The almost horizontal obliquus capitis inferior (OCI) is inserted on the transverse process of the atlas and originates from the spinous process of the axis (C2). It contributes to head movement related to fast visual exploration.
OCI is the biggest suboccipital muscle and is the 2nd strongest head rotator (after the sternocleidomastoid).
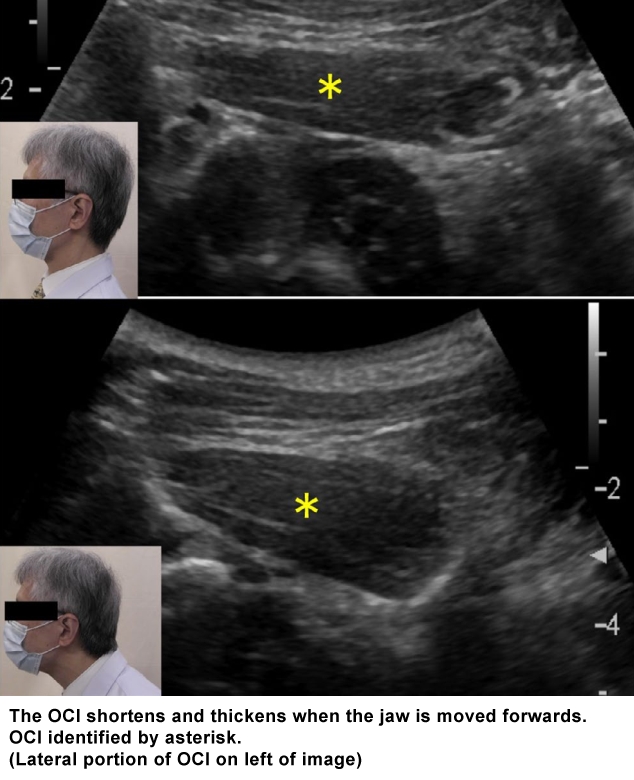
The depth from the skin to the superficial fascia of the muscle ranges from about 10 mm to over 35 mm. The muscle thickness also has a wide degree of variability, ranging from 10 to 20 mm, and when it contracts, its thickness increases and the length shortens.
From: Dr. Joe Muscolino. www.learnmuscles.com – art work Giovanni Rimasti
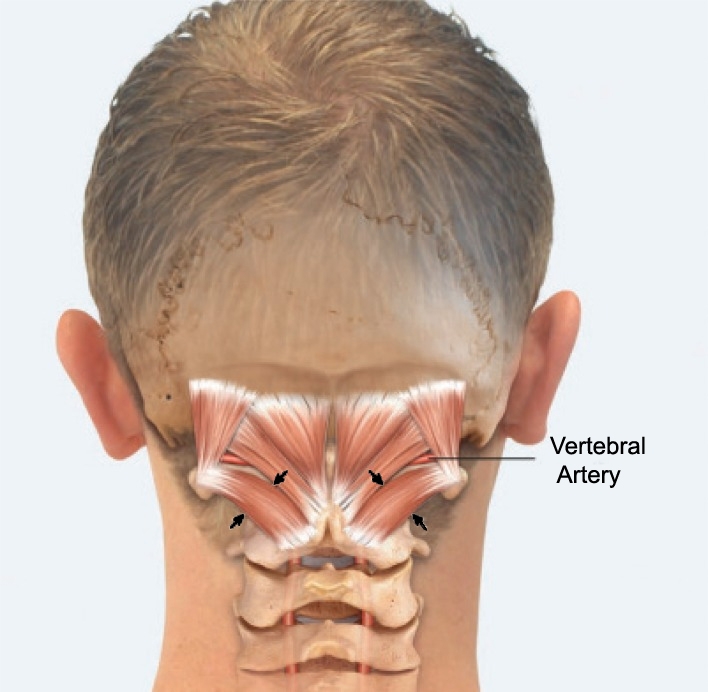
The muscle arises from the lateral mass of the atlas bone. It passes superiorly and posteriorly to insert into the lateral half of the inferior nuchal line on the external surface of the occipital bone.
Ultrasound Technique
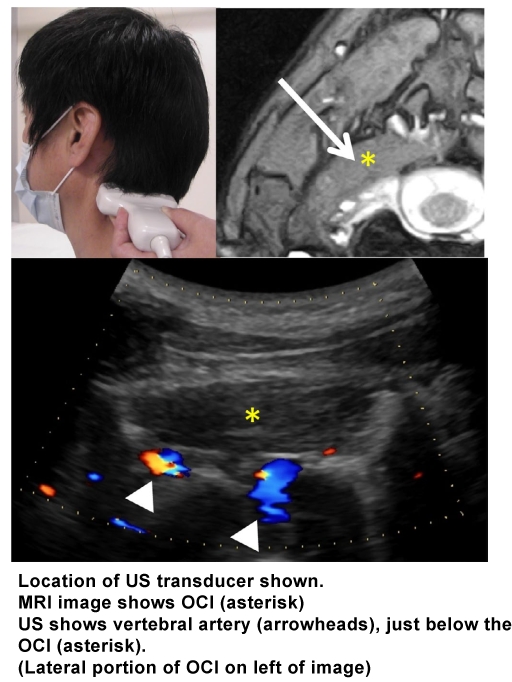
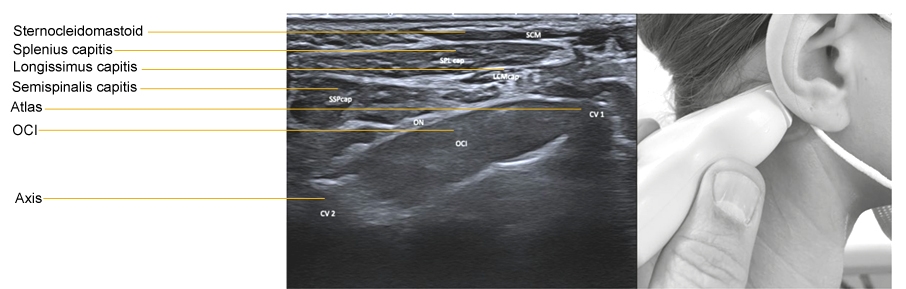
1. Place the convex transducer horizontally on the posterolateral neck at a level just below the tip of the mastoid process.
2. Rotate the dorsal end of the transducer a little downward, and turn the transducer a little in a rostral direction.
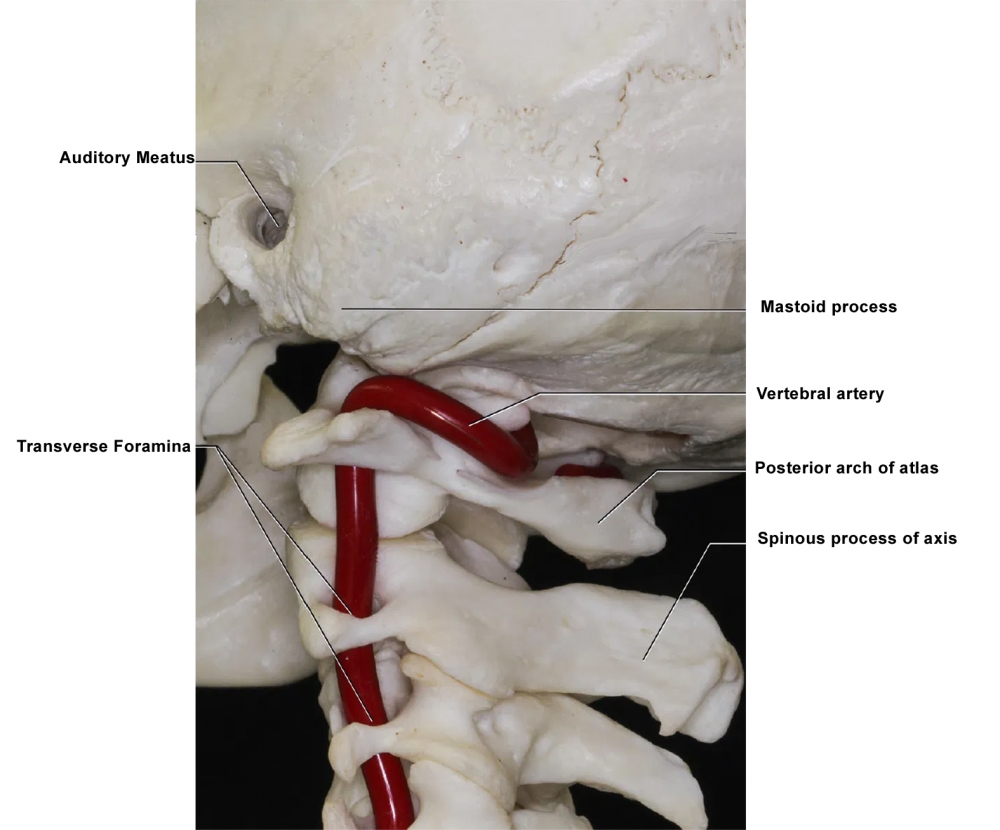
3. Identify the OCI. Normally, it is sausageâ€like, but may become ovoid in shape when it is hyperactive. The vertebral artery is just beneath the muscle. Confirm it with the color Doppler imaging. When the OCI is difficult to detect, because of intramuscular fibrosis the vertebral artery may help identify the muscle. There are occasionally other arteries superficial to the OCI.
4. Measure the approximate depth from the skin to the OCI and the muscle thickness before needle insertion in order to penetrate the muscle and not injure the vertebral artery.
6. After confirming the absence of any major artery along the expected needle path, insert the needle (27 gauge, 38 mm) from above the transducer. Direct the needle tip slightly downward so as to let the needle proceed within the ultrasound coverage area. Botulinum toxin is usually injected into medial and lateral portions of the muscle, but if the muscle is shortened by contraction its central portion may be the only site of injection.
 |
 |
 |
 |
From: Fietzek UM, Nene D, Schramm A, Appel-Cresswell S, Košutzká Z, Walter U, Wissel J, Berweck S, Chouinard S, Bäumer T. The Role of Ultrasound for the Personalized Botulinum Toxin Treatment of Cervical Dystonia. Toxins (Basel). 2021 May 20;13(5):365.
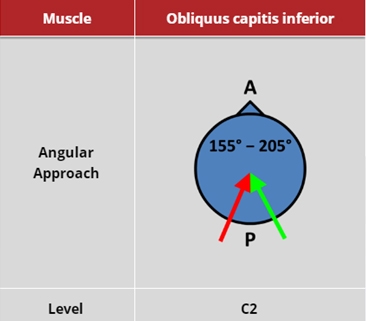
Three different approaches to injection of OCI
A: In plane technique
B: Out of plane technique
C: Sagittal approach: out of plane approach.
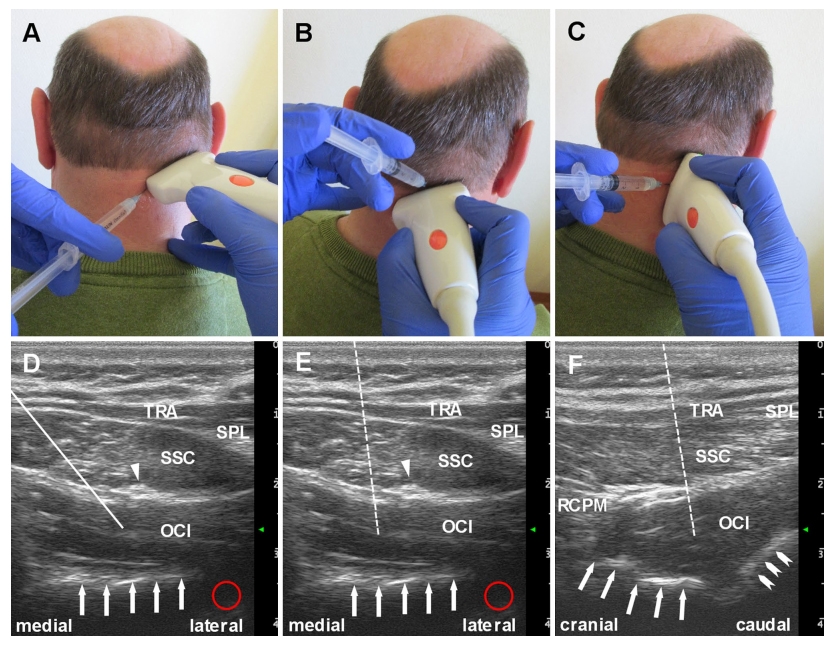
TRA: Trapezius; SPL: Splenius; SSC: Semispinalis capitis; RCPM: Rectus capitis posterior major
White arrows indicate bone; red circle indicates possible site of vertebral artery. Triangle: Greater occipital nerve
Dashed line (E and F) indicates potential path of the needle
From: Walter U, Dudesek A, Fietzek UM. A simplified ultrasonography-guided approach for neurotoxin injection into the obliquus capitis inferior muscle in spasmodic torticollis. J Neural Transm (Vienna). 2018 Jul;125(7):1037-1042.
(vv)OCI.mp4(tt)
(vv)OCIfietz.mp4(tt)
Segment 1: The initial positioning of the ultrasound probe at the patient’s neck is demonstrated. After visualization of the processus spinosus of vertebra C4 the ultrasound probe is shifted in cranial direction in order to display the OCI at the level of vertebra C1. Segment 2: For full display of the OCI muscle on axial imaging plane the ultrasound probe is shifted in medio-lateral direction and slightly twisted, moving the anterolateral part in an upwards direction.
Segment 3: For optimal display of the OCI muscle belly on sagittal imaging plane the ultrasound probe is rotated by 90 degrees.
Segment 4: The US-guided insertion of the injection needle (here connected to an electromyography machine) is presented. The needle tip is visible on the screen. Note the electromyography noise demonstrating dystonic activity of the OCI muscle. During the injection of the BoNT the electromyography noise disappears.
From: Walter U, Dudesek A, Fietzek UM. A simplified ultrasonography-guided approach for neurotoxin injection into the obliquus capitis inferior muscle in spasmodic torticollis. J Neural Transm (Vienna). 2018 Jul;125(7):1037-1042.