| EYE OF SAURON |
LOCATION
|
SAGITTAL T2 |
POST CONTRAST SAGITTAL |
Other features |
|


|
Commonly, Cervical>Thoracic.
Note that short segment lesions
are seen in 15% of patients.
Lesions frequently extend up
into the medulla1.

|
Spinal cord involvement is extensive,
with high T2 signal spanning at least three
vertebral segments, often many more
(known as a longitudinally extensive spinal
cord lesion).
Cord swelling is usually present in the acute phase.

From Ref 6
|
Rings/partial ring of enhancement.
Rings may be elongated or have shaggy borders3.

|
Bright spotty lesions are a specific features
of NMO and consist of marked T2
hyperintense (higher than CSF)
and T1 hypointense foci in the central grey
matter4.
Axial T2WI image shows “bright spotty lesions”
(BSLs) in the central area (A), and BSLs show low
signal on axial gadolinium-enhanced T1WI (B).
Axial T2WI shows several BSLs in the central and
peripheral area (C), and the BSL show low signal
ntensity on axial gadolinium-enhanced T1WI (D).

From Ref 3
|
| |
|
 
|


|
|
COMPARISON OF MOG, NMO AND MS
|
AXIAL T2 |
POST CONTRAST |
|
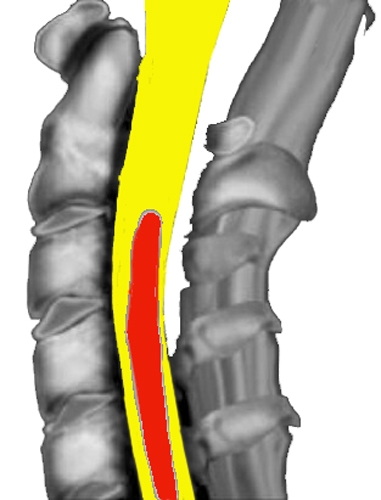
MOG: Sagittal T2-hyperintense line (white arrowhead) surrounded by hazier T2 hyperintensity
(yellow arrowheads)
On axial sequences, the T2 hyperintensity is highly restricted to the gray matter forming an H sign
(red arrowhead).
Postgadolinium sagittal images demonstrate no gadolinium enhancement.
NMO: Hyperintense extensive lesion with prominent swelling (yellow arrowheads) and axial T2
lesion with diffuse central signal abnormality not confined to gray matter (red arrowhead).
MS: Short T2-hyperintense lesion at the C2 level extending one vertebral segment in length
(yellow arrowhead) with accompanying faint ring enhancement (blue arrowhead).
On axial sequences, the lesion is located in the periphery of the cord in the right dorsal column
(red arrowhead).
|
Central (Predominantly gray matter)5
Both halves of the cord.

From: Ref 6.
|
Patchy gadolinium enhancement
involving central cord.
Ring/partial ring of enhancement3.

From: Ref 6.
|
 |

 From: Reference 4 From: Reference 4

|
 From: Reference 4 From: Reference 4 
|
References
1. Flanagan EP, Weinshenker BG, Krecke KN, et al. Short myelitis lesions in aquaporin-4-IgG-positive neuromyelitis optica spectrum disorders. JAMA Neurol 2015;72(1):81–7.
2. Lee MJ, Aronberg R, Manganaro MS, Ibrahim M, Parmar HA. Diagnostic approach to intrinsic abnormality of spinal cord signal intensity. Radiographics 2019;39(6):1824–39.
3. Yonezu T, Ito S, Mori M, et al. Bright spotty lesions" on spinal magnetic resonance imaging differentiate neuromyelitis optica from multiple sclerosis. Mult Scler J 2014;20(3):331–7.
4. Flanagan EP. Autoimmune myelopathies. Handb Clin Neurol. 2016;133:327-51. doi: 10.1016/B978-0-444-63432-0.00019-0. PMID: 27112686.
5. Mustafa R, Passe TJ, Lopez-Chiriboga AS, et al. Utility of MRI Enhancement Pattern in Myelopathies With Longitudinally Extensive T2 Lesions. Neurol Clin Pract 2021;11(5):E601–11.
6. Lopez Chiriboga S, Flanagan EP. Myelitis and Other Autoimmune Myelopathies. Contin Lifelong Learn Neurol 2021;27(1):62–92.